PERIO FOR THOUGHT - February 20, 2020
The definition of a hopeless tooth is, I dare say, somewhat elusive and ethereal. In fact, in the 2 decades of my career, the definition has been challenged numerous times. Traditionally, the prognosis of a hopeless tooth is granted to the one that got involved by the disease to the point that it is considered unbeneficial and/or even detrimental to leave it in place. As an example: a vertical fracture is often a clear indication for extraction.
In periodontology a dramatic vertical bone resorption, deep pockets associated with intrabony defects, degree III furcation, especially in the maxilla, endo-perio lesion, apex involvement, mobility degree III with attachment loss etc. have often been quoted as decisive factors in the prognosis of the tooth.
Understanding the criteria according to which a tooth should be extracted is a decisive factor when setting up a proper treatment plan. This is not only related to the fate of the tooth in question but also the adjacent ones. One of the points that had attracted, in the golden age of the 70s-90s, a significant interest from the research community was indeed the fate of the neighbouring teeth. This was even more complex as the evidence available was far from conclusive, conflicting data was published and, based on the actual knowledge, the evidence produced back then did not allow generalizability of the findings.
Yet, the clinical dilemma is very relevant. We’ve all faced a patient saying: “If it does not hurt, why should I have it removed?” Obviously, one of the responses, something I have heard many times, is suggesting the patient that that particular tooth might create harm to the neighbouring, healthy one.
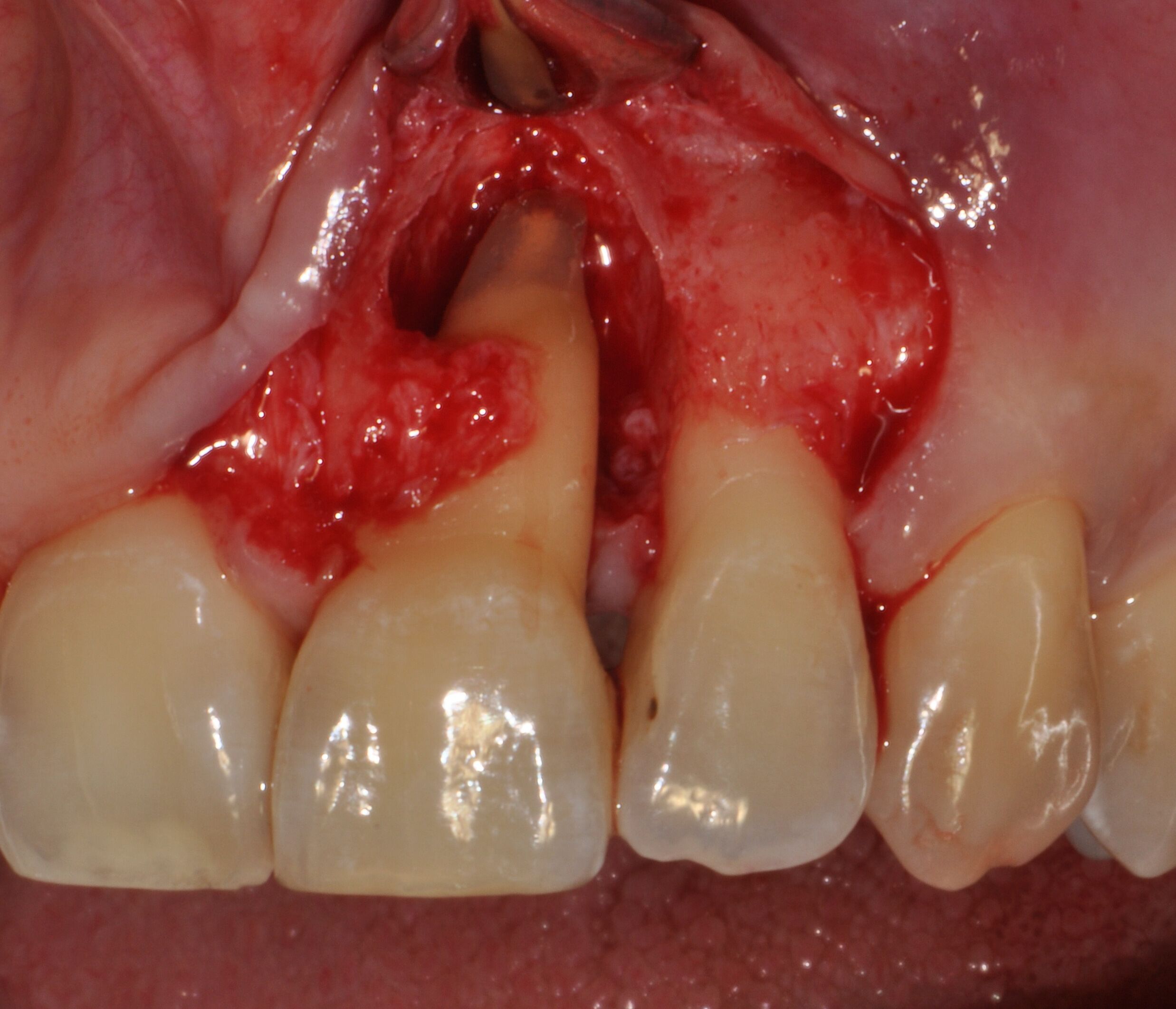 Intraoperative view of the surgical treatment of an upper left central incisor
Intraoperative view of the surgical treatment of an upper left central incisor
However, clinically and research-wise, we know that we can retain teeth with perio-apex involvement even in the long run. We have surely all seen enormous endo lesions healing following “just” a traditional, yet exceptional, ortograde endo treatment. In all fairness, I am sure all of us have cases that should have entered the category of hopeless, yet that are still in function after years.
I do wonder, over and over again, what would happen if we tried to keep every single tooth in the oral cavity at all costs, no matter what. In this thought experiment, our patient would also have access to the best clinicians and no particular financial limitation. All possible endo/restorative/perio treatments could be carried out. If this was the case, would it and in what way the treatment plan change? Now, back to reality and pragmatism: we treat our patient the best we can, and financial limitations have a significant and real impact on our treatment plan. Still, I cannot help myself but to question if I am doing the best in the interest of the patient when I am going for extraction.
Regretfully, I don’t have a clear answer to all these daily clinical dilemmas. Still, I do have some hope that with the passage of time and more trials published on complex defects, a strategy based on tooth conservation would be reinforced. In fact, a clear definition of the characteristics suggesting tooth extraction are changing year by year, and clinician by clinician.
Keeping the teeth in the mouth is our ethos. The goal of periodontology is to change the prognosis of questionable, and even sometimes hopeless, teeth. Hopeless is, actually, only the tooth that you have just extracted.


5-year post-treatment probing depth and intraoral periapical radiograph
P.S. Another story is the so-called "irrational-to-treat" tooth. This is a tooth that might not have, per se, the characteristics of severity that would make it fit the category of hopeless but because there is no point or little advantage in keeping the tooth (i.e. the only tooth in the area, with no opposing dentition, an isolated wisdom tooth, etc.) As such, the tooth is allocated in the category that needs extraction.